Appropriate use of available inpatient beds is an ongoing challenge for US hospitals. Historical capacity goals of 80% to 85% may no longer serve the intended purpose of maximizing the resources of space, staff, and equipment. Numerous variables affect the input, throughput, and output of a hospital. Some of these variables include patient demand, regulatory requirements, coordination of patient flow between various systems, coordination of processes such as bed management and patient transfers, and the diversity of departments (both inpatient and outpatient) in an organization.
Mayo Clinic Health System in the Southwest Minnesota region of the US, a community-based hospital system primarily serving patients in rural southwestern Minnesota and part of Iowa, consists of 2 postacute care and 3 critical access hospitals. Our inpatient bed usage rates had exceeded 85%, and patient transfers from the region to other hospitals in the state (including Mayo Clinic in Rochester, Minnesota) had increased. To address these quality gaps, we used a blend of Agile project management methodology, rapid Plan-Do-Study-Act cycles, and a proactive approach to patient placement in the medical-surgical units as a quality improvement initiative.
During 2 trial periods of the initiative, the main hub hospital (Mayo Clinic Health System hospital in Mankato) and other hospitals in the region increased inpatient bed usage while reducing total out-of-region transfers.
Our novel approach to proactively managing bed capacity in the hospital allowed the region’s only tertiary medical center to increase capacity for more complex and acute cases by optimizing the use of historically underused partner hospital beds.
Establishing an ideal number of staffed inpatient beds is a complex issue for health care organizations. Numerous factors, such as planned and predicted inflows into the hospital system, contribute to this challenge. Historically, bed demand for elective and other surgical procedures requiring an inpatient bed has been easier to predict than that for admissions from the emergency department, urgent care, and clinic visits [1]. Other variables, such as labor markets, space constraints, and equipment use, add to the complexity of predicting bed demand. Inadequate inpatient bed availability has led to emergency department crowding and, in turn, concern for the quality of services delivered [2, 3]. These factors combine to create a challenging operational workflow when managing inpatient bed usage [4, 5].
Our hypothesis centered on the strategic allocation of beds among various hospital sites. Specifically, we hypothesized that proactive bed assignment at tertiary centers for patients with presenting signs of severe illness who require specialized care unavailable at smaller sites will enhance regional health care provision. Concurrently, we hypothesized that optimizing the capacity at smaller hospitals by admitting patients with non-severe illness will improve patient distribution and thereby augment the ability of hospital systems to deliver comprehensive care throughout a health care region. To test this hypothesis, we developed a novel approach (via a combination of various methods) to bed hold to ensure that hospital beds were available for patients with severe illness (those requiring specialized services such as Cardiology, Neurosurgery, Orthopedic Surgery, Trauma Care, Interventional Radiology or Gastroenterology procedures) at the Mayo Clinic Health System (MCHS) hospital in Mankato, Minnesota, USA (MCHS-Mankato). This dual-pronged approach anticipates both unplanned, acute admission requirements and the ongoing need for beds for less critical cases. MCHS-Mankato is the only hospital that provides acute care, primary care, continuous emergency care, a level II nursery, critical care, advanced trauma care, and specialized medicine in southwestern Minnesota. Therefore, reducing or preventing transfers to outside of the region and providing care to patients at the right place and at the right time were important aims of our study. However, certain emergency situations required transfer to another tertiary hospital in which advanced care is provided.
The Admission Transfer Center (ATC) at MCHS acts as a critical node for patient distribution, operating like an air traffic control center to manage patient placement. The ATC, staffed by triage nurses at a centralized Southern Minnesota location, connects to all MCHS sites via an advanced information technology network. It uses data-driven strategies to facilitate timely transfers and improve patient flow, which contributes to operational efficiency. Additionally, its unique model provides a rich data source for investigating the dynamics of patient transfers, which thereby fosters various research opportunities.
The MCHS Southwest Minnesota region (SWMN) is based on a hub-and-spoke model that includes 2 acute care hospitals and 3 critical access hospitals. MCHS-Mankato is the only tertiary medical center and is the hub in this region. Four spoke hospitals in the region (Fairmont, St James, New Prague, and Waseca, Minnesota) serve patients with less severe illness. MCHS-Mankato consistently had greater than 95% occupancy and remained in diversion status on most days since the COVID-19 pandemic began because of a combination of increased demand, bed closures, staffing shortages, and other challenges. During the same period, tertiary hospitals throughout Minnesota also had high occupancy rates, which limited their capacities to accept patient transfers. These limitations resulted in previously unseen delays in hospital care throughout southwest Minnesota.
In SWMN, patients requiring care for severe illness and subspecialty care could often be served only at MCHS-Mankato. Therefore, these patients would be transferred out of the region when no inpatient beds were available at MCHS-Mankato. At the start of this project, the spoke hospitals in SWMN were not consistently reaching full occupancy. The historical method of admitting patients to MCHS-Mankato until full capacity was reached failed to make use of open spoke hospital beds for appropriate patients.
In the third quarter of 2021, MCHS-Mankato started the design and implementation of a project to optimize hospital bed management in SWMN. This project aimed to ensure the availability of beds for local patients with severe illness, maximize capacity opportunities in the surrounding spoke hospitals, and reduce out-of-region transfers. The spoke hospitals, all under the purview of MCHS leadership and operationally integrated via the ATC, were pivotal as key stakeholders in the formulation of our study design.
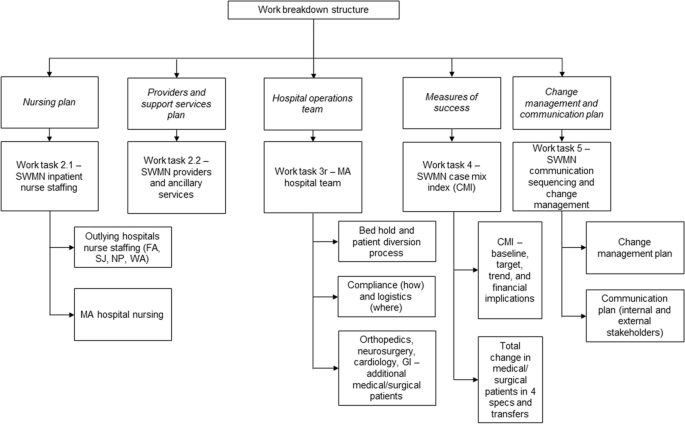
The initiative for optimizing hospital bed management was divided into 2 phases: phase 1, which comprised discovery (opportunity identification), planning, and proposal steps, and phase 2, which consisted of implementation. Through direct engagement with key stakeholders, phase 1 of the project followed the project engagement approach outlined in Table 1. This approach was closely aligned with Agile methodology and principles and our work breakdown structure (Fig. 1) to yield our overarching deliverables in the form of tasks or work buckets. In phase 2 of the project, 4 work streams were proposed after brainstorming sessions with subject matter experts and key stakeholders. The 4 work streams included the pre-admission process, transfer plan, updated admission guidelines, and updated diversion plan (Table 2). These work streams were led by respective operations, nursing, and executive partners. Each work stream was critical to ensuring that all aspects of hospital input were addressed in pursuit of optimizing bed management.
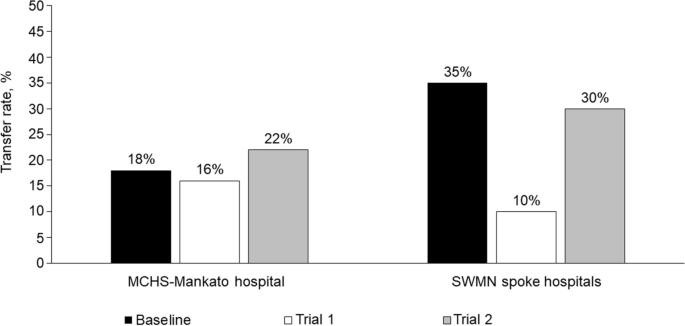
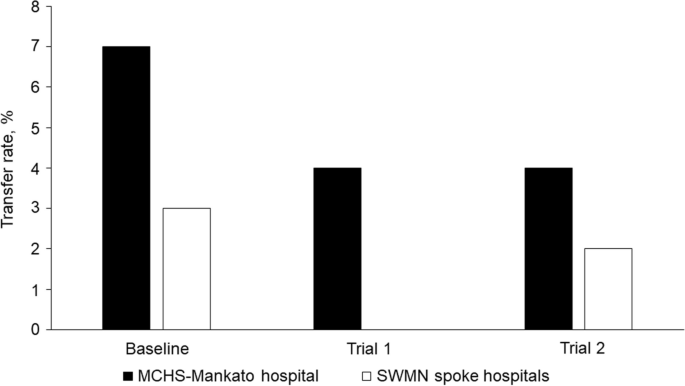
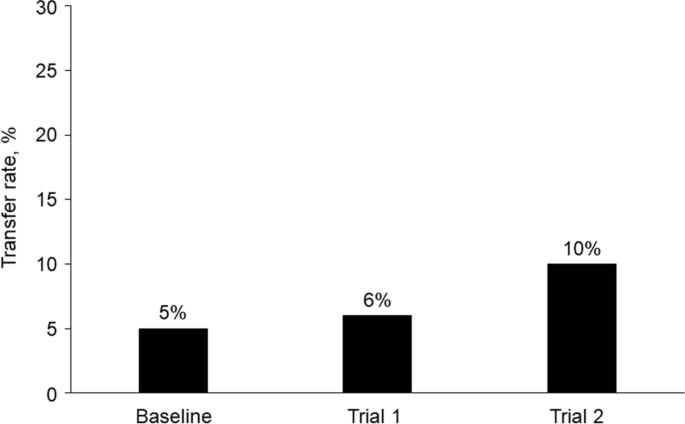
Considerable inpatient nurse staffing shortages occurred during trial 2, which did not occur during trial 1. This resulted in closure of an average of 22 inpatient beds per day (20% reduction) during trial 2, which further reduced hospital capacity. However, MCHS-Mankato continued to admit 97% of our average historical admission volume. During trial 2, the rate of all-cause transfers from MCHS-Mankato increased by 22% from baseline (Fig. 2), but the mean transfer rate of patients from MCHS-Mankato to Mayo Clinic in Rochester, Minnesota, decreased from a baseline of 7% to 4% (Fig. 3). Although service line admission volume did not increase during trial 2, the mean daily census for all 4 service lines increased from 0 beds at baseline to 30 beds after trial 2, despite inpatient capacity reduction. Parallel transfers from MCHS-Mankato to the SWMN spoke hospitals and SEMN hospitals increased from 5% at baseline to 10% during trial 2 (Fig. 4).
The complexity of treating patients requiring hospital care has been increasing, while the challenges of providing continuous staffing in hospitals have been mounting for health care organizations. Many recommendations on how hospitals can improve their performance despite these challenges have been proposed [6]. Improvements in patient flow and movement pathways, as well as care coordination through optimization of admission and discharge processes, are methods that can positively affect quality and patient care outcomes [7]. Intentionally delineating roles among hospital frontline staff and management teams has also shown positive results [8]. Our study used a novel strategy of combining some of these well-documented recommendations with new strategies to optimize our regional inpatient service, which routinely exceeds 85% capacity.
The PDSA cycle outcomes of the 2 implementation trials yielded results that supported our hypothesis. These findings suggest that hospital systems may benefit from proactively assigning beds for patients with severe illness at their tertiary centers and optimizing capacity at their smaller hospital sites by admitting patients without severe illness. Often, hospital systems will fill available capacity on a first-come, first-served basis. This approach prioritizes speed of admission and discounts matching patient needs with medical and surgical resource availability at the right location and time.
Research regarding the strategy of proactively transferring patients between acute care hospitals and non-acute care hospitals in a health system appears to be limited. However, some studies have reported that patients with complex conditions and who have been transferred to another hospital may have poor outcomes [9, 10]. Traditionally, patient transfers occur only after a tertiary hospital activates diversion procedures. Our findings suggest that identifying bed demand for patients with severe illness should not be limited to intensive and progressive care units only. Alternatively, a clearly delineated projection of bed demand for patients who require complex services must be considered when creating operational capacity designations.
Although our preliminary findings indicated a positive outcome of our quality improvement initiative, these findings were limited by an increase in bed shortages because of staffing constraints and fluctuating patient volumes in clinics, urgent care centers, and emergency departments. The bed shortages that occurred during the second implementation trial could have affected the integrity of our optimization project data. Increased barriers to inpatient bed access also challenged the enhancement of the exception criteria process, which remains an opportunity for improvement. Emergency medicine practitioners felt particularly challenged in finding recipient hospitals for patients in a timely manner. However, MCHS leadership helped reinforce the value of this project, which prioritized bed access for patients with severe illness and thereby reduced the risk of boarding or transferring critical care patients. Our analysis also lacked sufficient statistical power to establish significant differences. Despite these limitations, our results suggest that our project to optimize hospital bed management in a regional health care system had a generally positive effect.
Operational inefficiencies in the ATC and transfer delays posed some challenges. Future ATC flow enhancements and more robustly staffed ambulance services may help mitigate these issues. Our spoke hospitals were crucial for developing this process and were engaged partners in the trials. The primary challenge was ensuring timely patient transfers from the emergency department and managing the ATC operational flow. Envisaging further collaboration between the ATC and emergency medical service, we aim to use their expertise for process streamlining, enhancing the patient experience, and creating a more coordinated system in SWMN.
Future iterations of regional capacity optimization studies will most likely include analytical forecasts, such as inpatient service line demand beyond the current projection of 6 to 8 weeks [11,12,13,14,15,16,17]. Bed designations can remain fluid and responsive to analytical projections for months and even years and as hospital data analytics develop. A better understanding of population health needs and advanced at-home care options, including advanced digital health and telemedicine offerings, will affect future hospitalization needs and forecasting of inpatient bed usage.
Some hospital systems may benefit from proactively transferring patients to hospitals in their system that primarily serve patients without severe illness at an early time in the admission cycle and reserving beds at a larger tertiary medical center for patients with severe illness. The traditional approach of filling a hospital, activating diversion procedures, and then seeking alternative placement fails to maximize resource capabilities in a large regional system. As capacity constraints continue to strain hospital systems, innovative approaches to the admission process must be explored. Historical operational models that are relevant to only a single hospital fail to meet the demands resulting from contemporary resource constraints.
The data supporting the conclusions of this article are included within the article.